Health
Coronary Artery Disease
Stents
Health
Coronary Artery Disease
Stents
| Home
Health
Coronary Artery Disease
Stents
|
| Heart Attack | Coronary Artery Disease | Cholesterol | Stents | Heart Bypass Surgery |
|
Under Construction 
We are talking about coronary artery stents here.
Symptoms are usually checked out with a stress test and nuclear scan and an echo cardiogram. If a problem is indicated a coronary angiogram is usually recommended with a procedure called Cardiac Catheterization.
Stents are usually placed only if there is a 70% or more blockage.
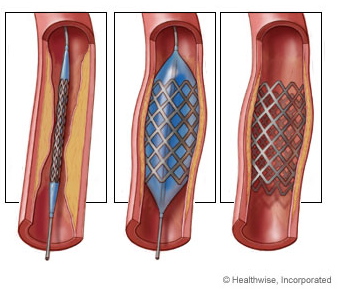
Stents are used with percutaneous coronary intervention (PCI)
or angioplasty. In it, a balloon-tipped tube (catheter)
is inserted into an artery and moved to the point of
blockage. Then the balloon is inflated.
See video
Although stented arteries have less chance of renarrowing than arteries opened with a balloon alone, in-stent restenosis (renarrowing) caused by tissue growth can still occur in more than 1 in 5 patients after stent placement. Recurrent angina may occur during the first couple of weeks following stent implantation. Often this is due to coronary spasm. When a vessel is dilated and stretched it becomes sore and inflamed much like a cut on the skin. Until this area heals the vessel may go into spasm due to it being raw and irritated.
Because stents expose foreign material to the blood stream, a small risk exists that a blood clot may develop in the stent, a process called stent thrombosis. These blood clots can occur many months and even years after stent implantation and may lead to a heart attack. A Duke University study found that there was a 1 in 40 chance of forming a blood clot in a drug-eluting stent when people were on blood-thinning medicine, but a 1 in 20 chance for people who stopped taking blood-thinning medicine after six months. Over time (about a year), cells like those on your artery wall will grow over the stent and many time the blood thinners can be discontinued then.
Blood Thinners
A 1999 study by the NIH was primarily to show that new antiplatelet drug Ticlopidine (trade name Ticlid) produced better outcomes. History:
Bypass surgery, Coronary artery bypass graft surgery (CABG), became common in the 70's to treat atherosclerosis Drug-eluting stents (DES): Sometimes there is excessive growth of tissue (scar tissue) at the edge of the stent causing restenosis. In early 2000 stents (called drug-eluting stents) that have medication on them to inhibit or prevent excessive tissue growth were introduced. Concerns about the safety of drug-eluting stents have received much publicity, primarily related to a small increase in the number of blood clots that develop within drug-eluting stents late (more than 1 year) after implantation. In December 2006, the US Food and Drug Administration convened a panel of cardiovascular experts to review drug-eluting stent safety data. The panel concluded that for many patients, such as those with uncomplicated medical histories who undergo elective stenting of simple coronary blockages, drug-eluting stents remain a safe and appropriate therapy. For others, such as those who have suffered an acute heart attack or those with multiple or complicated coronary blockages, current data are inadequate to determine whether drug-eluting stents are better or worse than bare-metal stents or coronary artery bypass surgery.
Older patients treated with drug-eluting stents had a 54 percent lower need for repeat treatments than those treated with bare-metal stents. Absorbable Heart Stent: In July, 2016 the U.S. Food and Drug Administration approved Abbott Laboratories' absorbable heart stent called Absorb. The current state of the art are drug-coated stents. The drug gradually seeps into the interior of the blood vessel to prevent growth of scar tissue that can cause clots to form. But recent research shows that the drug-coated stents are associated with serious adverse events, including death and heart attack, at a rate of 2% to 3% a year. The hope is that a dissolvable stent will reduce such problems. A 2008-person study, called Absorb III, found that 7.8 % of patients treated with the new device suffered "a major cardiac adverse event," a rate that was "clinically comparable" to the 6.1% rate for those treated with Abbott's drug-coated metal stent called Xience.
because Absorb leaves nothing behind it may provide significant long-term benefits, such as a restored vessel in a natural state and renewed possibilities for people treated with Absorb," said Dr. Charles Simonton, chief medical officer of Abbott Vascular in a statement. Sources: Google Search What Is a Stent? - American Heart Association Drug-Eluting Stents | Circulation - AHA Journals FDA Approves Abbott's Absorbable Heart Stent - WSJ Abbott's bioresorbable stent meets primary endpoint, but NEJM editorial raises questions | FierceBiotech What Are the Risks of Having a Stent? - NHLBI, NIH |